CORONAVIRUS DISEASE 2019 (COVID- 19 )
{{hitsCtrl.values.hits}}
31 March 2020 02:57 pm
Prepared by Dr. Mala Tudawe Consultant Haematologist (Concise version from the report of the WHO-CHINA joint mission on Coronavirus 2019) On 30 th December 2019, three Broncho alveolar lavage samples were collected from a patient with pneumonia of unknown etiology – in Wuhan Jinyintan Hospital. Real-time PCR (RT-PCR) assays on these samples were positive for pan-Beta coronavirus. Bioinformatic analyses indicated that the virus had features typical of the coronavirus family and belonged to the Betacoronavirus 2B lineage. Further tests showed the closest relationship was with the bat SARS-like coronavirus strain BatCov RaTG13, identity 96%. Typical crown-like particles were observed under transmission electron microscope (TEM) with negative staining. Post-mortem samples from a 50-year old male patient from Wuhan were taken from the lung, liver, and heart. Histological examination showed bilateral diffuse alveolar (those are the air filled spaces in the lungs) damage with cellular fibromyxoid exudates (this is a very thick liquid) filled in the alveolar. Basically the symptoms are like drowning in your own fluids as the air pockets are filled with thick fluid. Similar to acute respiratory distress syndrome (ARDS). From the confirmed cases reported as of 20 February 2020, the median age is 51 years, with the majority of cases (77.8%) aged between 30–69 years. Among reported cases, 51.1% are male, 77.0% and 21.6% are farmers or laborers by occupation respectively. Routes of transmission COVID-19 is transmitted via droplets and fomites (objects like clothes, utensils, furniture) during close unprotected contact with the affected. Airborne spread has not been reported for COVID-19 and it is not believed to be a major driver of transmission based on available evidence; however, it can be envisaged if certain aerosol-generating procedures are conducted in health care facilities. Fecal shedding (from stools) has been demonstrated from some patients, and viable virus has been identified in a limited number of case reports. However, the fecal-oral route does not appear to be a driver of COVID-19 transmission. In China, human-to-human transmission of the COVID-19 virus largely occurred in families. As COVID-19 is a newly identified pathogen, there is no known pre-existing immunity in humans. Based on the epidemiologic characteristics observed so far in China, everyone is assumed to be susceptible, although there may be risk factors increasing susceptibility to infection. Transmission in Wuhan Early cases identified in Wuhan are believed to be have acquired infection from a zoonotic source (animal source) as many reported visiting or working in the Huanan Wholesale Seafood Market. As of 25 February, an animal source has not yet been identified. Data on individuals aged 18 years old and under suggest that there is a relatively low attack rate in this age group (2.4% of all reported cases). Within Wuhan, no children were positive in November and December of 2019 and in the first two weeks of January 2020. Typical signs and symptoms: fever (87.9%), dry cough (67.7%), fatigue (38.1%), sputum production (33.4%), shortness of breath (18.6%), sore throat (13.9%), headache (13.6%), myalgia ( muscle pain)or arthralgia (bone pain) (14.8%), chills (11.4%), nausea or vomiting (5.0%), nasal congestion (4.8%), diarrhea (3.7%), and hemoptysis (bleeding from nose) (0.9%) , and conjunctival congestion-(red eyes) (0.8%). People with COVID-19 generally develop signs and symptoms, including mild respiratory symptoms and fever, on an average of 5-6 days after infection (mean incubation period 5-6 days, range 1-14 days). Most people infected with COVID-19 virus have mild disease and recover. Approximately 80% of laboratory confirmed patients have had mild to moderate disease, which includes non-pneumonia and pneumonia cases, 13.8% have severe disease –dyspnea (difficulty in breathing) with low blood O2 saturation. And 6.1% are critical (respiratory failure, septic shock, and/or multiple organ dysfunction/failure). Individuals at highest risk for severe disease and death include people aged over 60 years and those with underlying conditions such as hypertension, diabetes, cardiovascular disease, chronic respiratory disease and cancer. Disease in children appears to be relatively rare and mild with approximately 2.4% of the total reported cases. GRAPH Pattern of disease progression for COVID-19 in China Note: the relative size of the boxes for disease severity and outcome reflect the proportion of cases reported as of 20 February 2020. The size of the arrows indicates the proportion of cases who recovered or died. COVID-19 is not SARS and it is not influenza. It is a new virus with its own characteristics. For example, COVID-19 transmission in children appears to be limited compared with influenza, while the clinical picture differs from SARS. As the animal origin of the COVID-19 virus is unknown at present, the risk of reintroduction into previously infected areas must be constantly considered. 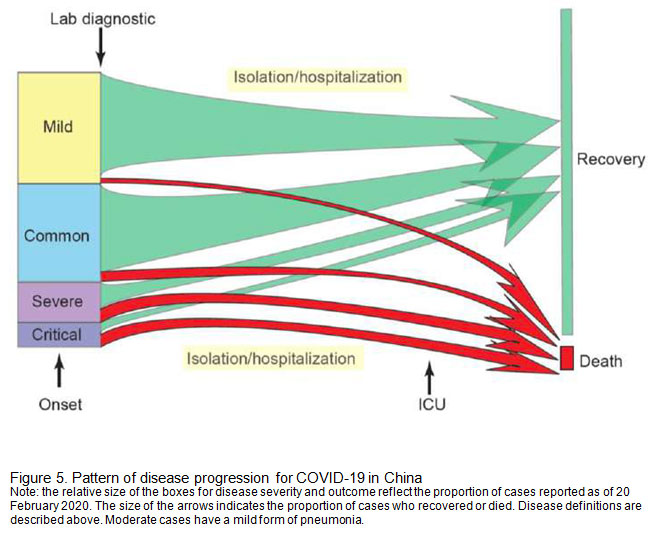 For countries with imported cases and/or outbreaks of COVID-19 (like in Sri lanka ) 01. Immediately activate the highest level of national Response; 02. Prioritize active, exhaustive case finding and immediate testing and isolation, painstaking contact tracing and rigorous quarantine of close contacts; 03. Fully educate the general public on the seriousness of COVID-19 and their role in preventing its spread; (e.g. the suspension of large-scale gatherings and the closure of schools and workplaces) 04. Immediately expand surveillance to detect COVID-19 transmission chains, by testing all patients with atypical pneumonias, conducting screening in some patients with upper respiratory illnesses and/or recent COVID-19 exposure Message to the public 1. Recognize that COVID-19 is a new and concerning disease, but outbreaks can be managed with the right response and that the vast majority of infected people will recover; 2. Begin now to adopt and rigorously practice the most important preventive measures for COVID-19 by frequent hand washing and always covering your mouth and nose when sneezing or coughing 3. Continually update yourself on COVID-19 and its signs and symptoms (i.e. fever and dry cough), because new information on this disease is accumulating every day; 4. Be prepared to actively support a response to COVID-19 in a variety of ways, including the adoption of more stringent ‘social distancing’ practices and helping the high-risk elderly population.
For countries with imported cases and/or outbreaks of COVID-19 (like in Sri lanka ) 01. Immediately activate the highest level of national Response; 02. Prioritize active, exhaustive case finding and immediate testing and isolation, painstaking contact tracing and rigorous quarantine of close contacts; 03. Fully educate the general public on the seriousness of COVID-19 and their role in preventing its spread; (e.g. the suspension of large-scale gatherings and the closure of schools and workplaces) 04. Immediately expand surveillance to detect COVID-19 transmission chains, by testing all patients with atypical pneumonias, conducting screening in some patients with upper respiratory illnesses and/or recent COVID-19 exposure Message to the public 1. Recognize that COVID-19 is a new and concerning disease, but outbreaks can be managed with the right response and that the vast majority of infected people will recover; 2. Begin now to adopt and rigorously practice the most important preventive measures for COVID-19 by frequent hand washing and always covering your mouth and nose when sneezing or coughing 3. Continually update yourself on COVID-19 and its signs and symptoms (i.e. fever and dry cough), because new information on this disease is accumulating every day; 4. Be prepared to actively support a response to COVID-19 in a variety of ways, including the adoption of more stringent ‘social distancing’ practices and helping the high-risk elderly population.
Leave a reply
Reply To:
Name - Reply Comment





Comments